Clear Cell Hidradenoma: Report of three cases
Clear cell hidradenoma is a benign eccrine gland tumour with a rare incidence of malignant transformation. It is more commonly seen in adult females in the second to fifth decades. Head and face are the most common sites. On histopathology. Tumour shows periodic acid–Schiff-positive clear cells and polyhedral cells. The recurrence rate is low if the lesion is completely excised. Here, we report three cases of clear cell hidradenoma presenting as a solitary nodule on the neck, scalp, and chest.
Keywords: Clear cell hidradenoma, eccrine, sweat gland
Introduction
The first case is a 30-year-old female who presented with an asymptomatic. Slow-growing lesion over the nape of the neck for a 3-year duration. Associated with bleeding on trauma or manipulation. There was no history of preceding trauma. The patient underwent excision of the lesion one year prior to presenting to us followed by recurrence. Cutaneous examination of the patient revealed a solitary erythematous nodule of 2 cm in diameter. On the nape of the neck with crusting on the surface of the lesion. (Figure a)
 Figure 1
Figure 1
Figure 1: (a) solitary erythematous, firm nodule of 2 cm in diameter with crusting on the surface over the nape of the neck. (b) single erythematous nodule of 0.5 cm diameter on the scalp with minimal crusting. (c) single, sessile, indurated, skin-colored nodule with the bosselated surface on the left side of the chest.
The second case is a 58-year-old male who presented with a small. Asymptomatic solitary lesion on the scalp for a 3-month duration. There was a history of slight serous discharge from the lesion with crust formation. Cutaneous examination of the patient revealed a single erythematous nodule of ½-cm in diameter. On the scalp with minimal crusting [Figure 1]b.
The third case is a 60-year-old male who presented with a single slow-growing asymptomatic lesion. On the chest for 2 years without a preceding history of trauma or bleeding on manipulation. Cutaneous examination showed a single, sessile, indurated, skin-colored nodule on the left side of the chest [Figure 1]c.
There was no evidence of regional lymphadenopathy in any of the three patients. Systemic examination and laboratory investigations of all the patients did not reveal any abnormality.
All of them underwent surgical excision of the tumor. Histopathological examination with H & E stain in all three cases revealed a well-circumscribed. Nonencapsulated dermal tumor with solid and cystic areas along with grenz zone [Figure 2]a]. Higher magnification showed two types of cell. Clear cell showing clear cytoplasm with eccentric nuclei and polyhedral cells with slightly basophilic. Finely granular cytoplasm and few mitotic figures. Intervening stroma showed dense hyalinized collagen [Figure 2]b and [Figure 3]a.
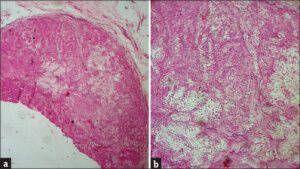 Figure 2
Figure 2
Figure 2: (a) Well-circumscribed, nonencapsulated dermal tumor with solid and cystic areas along with grenz zone (H and E, ×40). (b) Clear cells showing clear cytoplasm with eccentric nuclei and polyhedral cells with basophilic cytoplasm (H and E, ×100)
 Figure 3
Figure 3
Figure 3: (a) Two types of cell: clear cells and polyhedral cells with slightly basophilic. Finely granular cytoplasm, and few mitotic figures (H and E, ×400). (b) Periodic acid–Schiff-positive clear cells (periodic acid–Schiff, ×400)
Clear cells were periodic acid–Schiff (PAS) positive and diastase labile due to their glycogen content [Figure 3]b.
There was no evidence of cellular atypia, atypical mitoses, and perineural or lymphovascular invasion and necrosis, suggestive of malignancy. Immunohistochemistry was not done in any of the patients as the diagnosis was definitive on histopathology.
Discussion
CCH is a rare histologically distinct tumor of the sweat gland duct. Found mainly in adults with a female preponderance. It was first described by Liu in 1949 as clear cell papillary carcinoma of the skin. Subsequently, it was reported under various designations. And the recent literature prefers the term CCH. Nodular hidradenoma, or solid and cystic hidradenoma and eccrine acrospiroma.
It usually presents as a slowly enlarging, single, asymptomatic, firm tumor, or nodule, 5–30 mm in size. And may be attached to the overlying epidermis. Some tumors discharge serous material while others tend to ulcerate.
Although traditionally regarded as displaying eccrine differentiation. It is now accepted that tumors can show either eccrine or apocrine differentiation.
The histopathological appearance of CCH is very typical. Characterized by two types of cells such as eosinophilic cells and clear cells along with duct-like cystic spaces lined by low cuboidal cells. Immunohistochemical analysis is not required in routine. Practice since most cases can be easily and reliably diagnosed with hematoxylin- and eosin-stained sections. Clear cells contain a variable amount of glycogen within their cytoplasm, unaccompanied by lipid material. Which is responsible for their clear component as well as for PAS positivity and diastase lability.
On immunohistochemistry, CCH shows reactivity for P63. Keratin, epithelial membrane antigen, carcinoembryonic antigen. S-100, and vimentin but negativity for alpha-smooth muscle actin (α-SMA), CD-10, estrogen receptors, and progesterone receptors.
Although rare, malignant transformation of CCH is seen in 6.7% of cases. The moma. The patient with this condition has an excellent prognosis. Recurrence is rare if the lesion isalignant counterpart, termed CCH or malignant CCH. Is exceedingly rare and is characterized by infiltrative borders. Cellular atypia, and numerous abnormal mitotic figures. In adults, one also has to rule out the possibilities of metastatic renal cell carcinoma and clear cell variety of squamous cell carcin completely excised.
We are reporting these cases as apart from one patient who had the tumor on the head and face region. Two patients had the tumors on less common sites like the neck and chest.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity. But anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.